Endometrial ablation is a surgical procedure that is an alternative to the mating of the uterine cavity. The essence of the operation is the complete or occasional partial removal of the lining of the uterus. The integrity of the internal body is not disturbed during the surgical intervention, which contributes to the further resumption of the menstrual cycle. The gynecologist prescribes this manipulation to women only if necessary, if the drugs are unable to overcome the disease.
Features of the method
Features of the method of endometrial ablation (resection or excision) are the complete removal of the uterine mucosa, which is carried out without the use of classical surgical tools, and with the help of modern painless methods.
The advantage of ablation is that the doctor does not need to make additional incisions and other manipulations, access to the endometrium is made directly through the cervical canal. When resection, it is necessary to remove the mucosa layer of the uterus: basal and functional layers with all tumors, including pathological and tumor. Very often the subject area of the muscle shell is also excised. Doctors cut 3 to 6 millimeters of tissue into thickness.
The remote mucosa layer is no longer sent to histological diagnosis, as its cells during the operation undergo irreversible destruction. If the doctor will use an electric loop, there is a possibility of obtaining suitable tissue samples for laboratory tests.
Types of endometrial ablation
Are currently being resectioned using modern technology. To remove the inner mucosa of the uterus used to contact or contactless laser light (photodynamic therapy), bipolar electroscalpel (the tool can be in the form of a ball, barrel, loop, roller). Electro-ablation with the help of a roller doctor classify the so-called “gold standard” and use it as a method of therapy for pathological changes of the uterine mucosa layer.
Other types of ablation include microwave (microwave exposure to areas of the mucous membrane), cryoablation (liquid nitrogen is pumped into the uterine cavity and manipulation), hydrothermoblation (as a result of surgery there is a contact temperature burn of the uterine mucosa). The procedure can be carried out with the help of an electrode, which will serve radiofrequency waves, causing instant coagulation of mucous membrane proteins.
Endometrial destruction treatment is also carried out using a hysteroscope, which is injected into the uterine cavity. The hysteroscope has an attached camera and is a light source, making it easier to carry out the surgery. The most popular treatment for many gynecological diseases, including endometrial destruction, is hysteroresecoccal ablation of the mucous membrane. The technique allows the specialist during the manipulation to assess the endometrium and monitor the correctness of the procedure.
Indications and contraception
The procedure should be carried out in the form of recurrent bleeding from the uterus, which affects women over the age of 35. If the medical treatment of metrorragia does not work, there is a need for endometrial ablation. In the recurrent hyperplasticity of the lining of the uterus, which occurs in patients before the onset of menopause and during it, it is necessary to resort to the exation of the mucosa layer. Often the procedure is prescribed as an alternative to radical surgical technique, namely hysterectomy.
If hormonal treatment is not possible for a woman, the gynecologist recommends resection.
Contradictions of manipulation:
- cancer of the mucosa layer of the uterus or internal organ;
- suspicions of malaginization of hyperplised tissues;
- uterine prolapse;
- acute diseases of the genitourinary system;
- Sexually transmitted diseases;
- blood clotting disorders.
If the patient has exacerbated chronic diseases or increased body temperature, the surgery should be postponed. In endometriosis it is not recommended to do the ablation. If a woman is diagnosed with uterine fibroids, the excision can be carried out if the nodes in diameter do not exceed 5 centimeters, and the increase of the internal organ is observed no more than 3 months.
Ablation Excision of the lining of the uterus is a surgical intervention, as a result of which the patient should remain hospitalized for 2-3 days. Before the procedure, the patient should be examined by a gynecologist and take tests of urine, blood, blood clotting, smears. The state of the heart and blood vessels is necessarily assessed and the endocrine status is determined. The expediency of testing and a full diagnosis of the body is to exclude cancer pathologies, which can cause bleeding and other negative side effects during surgery. Manipulation is prescribed on 5-8 days of the menstrual cycle because the mucous layer of the organ at this time has the smallest thickness. If the patient has irregular periods or does not have them at all, the day of surgery is determined by ultrasound. Often before manipulation is prescribed hormonal drugs, they create favorable conditions for the complete excision of the endometrium.
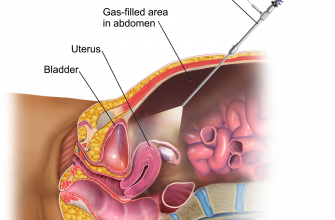
Resection of the mucous membrane is performed under general or spinal anesthesia. The patient is located on the gynecological table in a certain position, it is called the position of Trendelenburg (the man lies on his back at a slope of 45 degrees with a raised pelvis) to reduce the pressure on the pelvic organs and smooth the bends of the uterus. In this position, the surgeon has full transvaginal access to the endometrium.
The cervix is fixed with special forceps, then the cervical canal expands with Ager’s toolkit. When using a hysteroscope, the doctor conducts a check-up of the uterus. If there is a suspicion of malagnoization of sites, it is advisable to do a targeted biopsy. Sometimes it is advisable to use an irrigation system that will create volume in the uterine cavity for the effectiveness and painlessness of the operation. When the manipulation comes to an end, the patient will be under the supervision of a specialist for 3-4 hours. If the woman does not have complaints about her health, she may be discharged from the hospital on the same day.
Doctors are afraid of complications, so they insist on 2-3 days of hospitalization. The maximum duration of hospitalization depends on the complications and the clinical situation in which the patient found herself.
Risks and possible complications
Risks of surgery include non-compliance with methodological technique and the need to use anesthesia. An extremely dangerous complication is the perforation of the wall of the inner organ by a catheter or electrode. In hysteroresescopic ablation, the risk of perforation is much lower, as the specialist during the operation can control the location of the toolkit. After surgery, the following complications may arise: the neuma inflammatory process in the uterus; heavy bleeding caused by damage to large vessels (blood discharge from the uterus after surgery is considered normal in the first 10 days, then you should seek medical attention); violation of the functions of adjacent organs (maybe due to the heating of the mucous during manipulation); burns of the vaginal walls and cervical canal (appear as a result of unobserved surgical intervention techniques).
After the procedure, the lower abdomen may ache, pull in the lower back, vomit a little, but only for 24 hours after ablation. This symptom speaks of an early recovery period and is the body’s response to the excision of the endometrium. Remote complications after surgery are considered: obstruction of the cervical canal and blue-acting. If there is a high risk of blue-hued, the doctor recommends that the patient install the Mirena spiral in the uterus. If the bleeding from the uterus resumes after 2-3 months, it is worth contacting a gynecologist. This fact may indicate that the endometrium has been completely removed.
Ablation and Reproductive Health
If a woman wants to have children, ablation will be carried out so that the patient regained the menstrual cycle (the destruction is completed by 1 centimeter above the edge of the internal yawn of the organ). In this case, menstruation will recover, but it will be meager and short-lived.
The patient of reproductive age, agreeing to ablation, does not lose the possibility of conceiving a child. During manipulation does not disturb the ovulatory function of the ovaries, sometimes the doctor can keep part of the mucous, which allows many women to feel all the charms of motherhood.
Of course, the excision of the mucous can lead to infertility, if the specialist disparages the operation or will be weakened in the patient. That is why before the procedure the doctor reports about possible risks.
Useful links:



Hysterectomy is the suggestion of the medical professional to me so the 3 big fibroids in my uterus are eliminated. But by sticking to the fibroids treatment plan “Gαmdοt Sυnυ” (Gοοgle it), 80% of fibroid tumors are completely gone or has shrunk. I am having a normal period at this point and the discomfort when I am having it is bearable to none.
My wife had to have this procedure, she used to bloody the sheets every month. Every thing is Ok now.
omg this is me .. previous heavy/flooding painful periods now I’ve had 22days of bleeding feeling so weak n dizzy my doctor give me Utovlan 2day.. I think this procedure wud help me.
the doctor claims there is no pain discharge, bleeding or pain after the procedure. BULLFRICKENSHIT!
I had this done this morning and I’m here to tell you that the pain is fierce. Totally worth it for the objective of ending my monthly torture cycle but I am bleeding like a light period,cramping like back labor and pins n needles / burning.
take all the pain medicine they offer you, seriously. I’m tough but this pain is no joke.
I got this done a few days ago. I am cramping and a bit sore. But well worth it. Before this, I was bleeding everyday since August 2017. Sometimes right into my running shoes, get up in the middle of the night and bed was soaked, wearing depends because of the amount of blood loss. I lost my job because I couldn’t concentrate due to lack of iron.. because of so much blood loss.. I was always having to go home due to leaking or dizziness . My relationship was suffering because I was grumpy worried and my husband bless his heart was trying to be understanding but how could he. In and out of hospital because I was getting sick because of lack of blood. The doctors put me on iron pills and Tranexamic acid 500 mg 2x 3 times a day. Nothing was working. This procedure is not barbaric this saved my life! I am now recovering and I already feel better then I have in years. More alive! I recommend this to any woman who does not want to have kids and is going through major pain and suffering and anything close to what I went through. You don’t have to suffer like your mother or grandma’s did!! Getting it was the best thing for me and maybe for you too!